High Blood Pressure or hypertension occurs when your blood pressure or the force of your blood pushing against the walls of your blood vessels is consistently high. As a result, your heart and blood vessels have to work harder to pump blood and make them work less efficiently. Over time, this can lead to tissue damage inside the arteries. This can put a person at risk for heart attack and stroke. High blood pressure often has no symptoms and is also known as the silent killer. There are different types of hypertension from primary hypertension to resistant hypertension. If your blood pressure is persistently high, you must get tested and start treatment. (Also read: Hypertension: Simple tips to control blood pressure in the middle of a cold spell
“Chronic elevation of blood pressure in the systemic arteries above 140 mmHg is referred to as hypertension or systemic arterial hypertension. However, the Indian Guidelines on Hypertension IV (IGH IV) defines it as hypertension. hypertension is a systolic blood pressure (SBP) above 140 mmHg and/or a diastolic blood pressure (DBP) of 90 mmHg.The ACC/AHA guidelines have changed the range to 130/80,” says Dr. RBM Makkar, Senior Diabetes Physician and RSSDI President.
Dr. Makkar talks about the different types of hypertension and how to manage them while interacting with HT Digital.
TYPES OF HIGH BLOOD PRESSURE
1. Primary hypertension
It is usually asymptomatic and identified by routine blood pressure checks or community screening. Mostly unaware of their condition, Indian patients with undiagnosed primary hypertension. Therefore, the Ministry of Health and the Family Welfare Guidelines indicate that patients with risk factors such as obesity, diabetes, history of cardiovascular disease, people over 60 years of age, and current smokers Medicines should be checked periodically.
2. Secondary hypertension
Often the result of a known cause of sudden worsening of BP. It is a secondary diagnosis for conditions such as obstructive sleep apnea, hyperaldosteronism, renal vascular hypertension, and renal disease (OSA). About 5–10% of cases of hypertension may develop secondary hypertension, of which 2-3% are renal parenchymal hypertension and 1-2% are renal vascular.
3. Gestational hypertension
It is a condition that affects pregnant women and increases the risk of maternal death and birth defects. It may occur with or without a diagnosis of preeclampsia.
4. White coat hypertension
Also known as isolated clinic hypertension, it is characterized by elevated in-office blood pressure readings but normal out-of-office readings. Diagnosis of white coat hypertension is indicated by ambulatory blood pressure monitoring. White coat hypertension occurs in patients whose office BP levels are at least 20/10 mmHg higher than their emergency values. Younger individuals in Indian patients have a higher risk of developing white coat hypertension than older adults.
5. Drug-resistant hypertension
When three or more antihypertensive drugs, including diuretics, fail to control a patient’s hypertension despite treatment, nonadherence and suboptimal antihypertensive therapy Means are excluded as the cause. These patients were later diagnosed with treatment-resistant hypertension. It affects up to 10% of people and is associated with a higher risk of cardiovascular disease, organ damage, and all-cause mortality.
HOW TO MANAGE HIGH BLOOD PRESSURE
1. To select the best medication to control hypertension, the individual patient profile and response to treatment must be considered.
2. ARBs (Angiotensin receptor blockers) may be used alone or in combination with CCBs (Calcium channel blockers) to lower blood pressure in patients with diabetes.
3. ARB and CCB combination therapy is recommended in the treatment of hypertensive patients to improve blood pressure control, reduce the risk of problems, and improve patient adherence.
4. Combination therapy must be recommended in patients at risk for cardiovascular disease, renal disorders, or cerebrovascular disorders to reduce patient mortality.
5. Based on the selection of therapeutic agents and their risk profile, monitoring of serum electrolytes, potassium and creatinine levels, as well as periodic assessment of renal function, is recommended. for hypertensive patients with diabetes.
6. For kidney and cardiovascular protection in people under 60 years of age, blood pressure should be kept below 130/80 mmHg in patients with CKD.
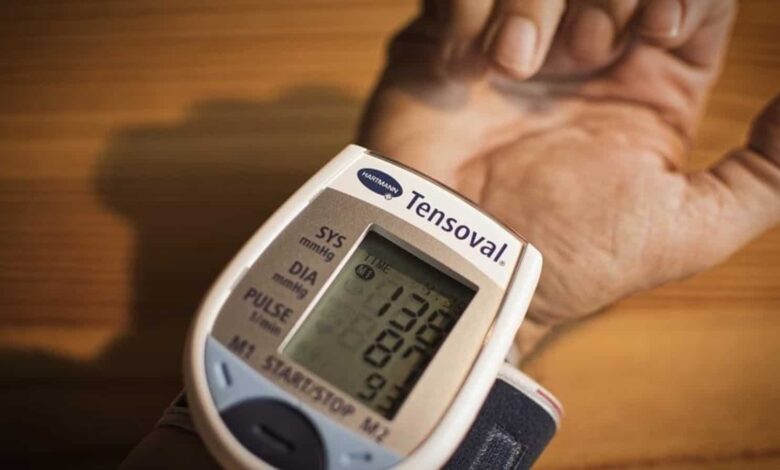
7. People with diabetes and hypertension should have their blood pressure monitored 24 hours to keep their readings between 120 and 130 mmHg. A digital device may be preferred for measurements taken at home, but an aneroid sphygmomanometer should be used instead. Age and comorbidities affect blood pressure thresholds.